
Below is a letter signed by 76 doctors in the UK, to the Medical and Healthcare products Regulatory Agency (MHRA) and other U.K. Government officials. This letter lays out comprehensive reasons why the recent U.S. FDA decision authorizing COVID vaccinations in infants and young children must not happen in the UK. The letter is well-sourced and accurate. Let us hope that mainstream media here in the USA and the UK report on this letter in an unbiased fashion.
I have not changed or added anything to this letter except that everything I write or copy and paste is put through a professional grammar-checking software, so some words and sentences may be corrected or changed. They shall mean and seam the same and so not alter the meaning of the letter in any way.
the letter continues)
We are writing to you urgently concerning the announcement that the FDA has granted an Emergency Use Authorization for both Pfizer and Moderna COVID-19 vaccines in preschool children.
We would urge you to consider very carefully the move to vaccinate ever younger children against SARS-CoV-2, despite the gradual but significant reducing virulence of successive variants, the increasing evidence of rapidly waning vaccine efficacy, the increasing concerns over long-term vaccine harms, and the knowledge that the vast majority of this young age group have already been exposed to SARS-CoV-2 repeatedly and have demonstrably effective immunity. Thus, the balance of benefit and risk which supported the rollout of mRNA vaccines to the elderly and vulnerable in 2021 is inappropriate for small children in 2022.
We also strongly challenge the addition of COVID-19 vaccination into the routine childhood immunization program despite no demonstrated clinical need, known and unknown risks (see below) and the fact that these vaccines still have only conditional marketing authorization.
It is noteworthy that the Pfizer documentation presented to the FDA has huge gaps in the evidence provided:
- The protocol was changed mid-trial. The original two-dose schedule exhibited poor immunogenicity with efficacy far below the required standard. A third dose was added by which time many of the original placebo recipients had been vaccinated.
- There was no statistically significant difference between the placebo and vaccinated groups in either the 6–23-month age group or the 2-4-year-olds, even after the third dose. Astonishingly, the results were based on just three participants in the younger age group (one vaccinated and two placebo) and just seven participants in the older 2–4-year-olds (two vaccinated and five placebo). Indeed, for the younger age group the confidence intervals ranged from minus-367% to plus-99%. The manufacturer stated that the numbers were too low to draw any confident conclusions. Moreover, these limited numbers come only from children infected more than seven days after the third dose.
- Over the whole period from the first dose onwards (see page 39 Tables 19 and 20), there were a total of 225 infected children in the vaccinated arm and 150 in the placebo arm, giving a calculated vaccine efficacy of only 25% (14% for the 6-23 months, and 33% for 2-4s).
- The additional immunogenicity studies against Omicron, requested by the FDA, only involved a total of 66 children tested one month after the third dose (see page 35).
It is incomprehensible that the FDA considered that this represents sufficient evidence on which to base a decision to vaccinate healthy children. When it comes to safety, the data are even thinner: only 1,057 children, some already unblinded, were followed for just two months. It is noteworthy that Sweden and Norway are not recommending the vaccine for 5-11s and Holland is not recommending it for children who have already had COVID-19. The director of the Danish Health and Medicines Authority stated recently that with what is now known, the decision to vaccinate children was a mistake.
We summarize below the overwhelming arguments against this vaccination.
A. The extremely low risk from COVID-19 in young children
- In the whole of 2020 and 2021, not a single child aged 1-9 died where COVID-19 was the sole diagnosis on the death certificate, according to ONS data.
- A detailed study in England from March 1st 2020 to March 1st 2021 found only six children under 18 years died with no co-morbidities. There were no deaths aged 1-4 years.
- Children clear the virus more easily than adults.
- Children mount effective, robust, and sustained immune responses.
- Since the arrival of the Omicron variant, infections have been generally much milder. That is also true for unvaccinated under-5s.
- By June 2022 it is now estimated that 89% of 1-4-year-olds had already had SARS-CoV-2 infection.
- Recent data from Israel show excellent long-lasting immunity following infection in children, especially in 5-11s.
B. Poor vaccine efficacy
- In adults, it has become apparent that vaccine efficacy wanes steadily over time, necessitating boosters at regular intervals. Specifically, vaccine efficacy has waned more rapidly against the latest Omicron variants.
- In children, vaccine efficacy has waned more rapidly in 5-11s than in 12-17s, possibly related to the lower dose used in the pediatric formulation. One study from New York showed efficacy against Omicron falling to only 12% by 4-5 weeks and to negative values by 5-6 weeks post the second dose.
- In the Pfizer 0-4s trial, the efficacy after two doses fell to negative values, necessitating a change to the trial protocol. After a third dose there was a suggestion of efficacy from 7-30 days but there is no data beyond 30 days to see how quickly this will wane.
C. Potential harms of COVID-19 vaccines for children
- There has been great concern about myocarditis in adolescents and young adults, especially in males after the second dose, estimated at one per 2,600 in active post-marketing surveillance in Hong Kong. The emerging evidence of persistent cardiac abnormalities in adolescents with post-mRNA vaccine myopericarditis, as demonstrated by cardiac MRI at 3-8 months follow-up, suggests this is far from ‘mild and short-lived’. The potential for longer-term effects requires further study and calls for the strictest application of the precautionary principle in respect of the youngest and most vulnerable children.
- Although post-vaccination myocarditis appears to be less common in 5-11-year-olds than in older children, it is, nonetheless, increased over baseline.
- In the Pfizer study, 50% of vaccinated children had systemic adverse events, including irritability and fever. Diagnosis of myocarditis is much more difficult in younger children. No troponin levels or ECG studies were documented. Even a vaccinated child in the trial, hospitalized with fever, calf pain and a raised CPK, had no report of D-dimers, anti-platelet antibodies or troponin levels.
- In Pfizer’s 5-11s post-authorization conditions, it is required to conduct studies looking for myocarditis and is not due to report results until 2027.
- Of equal concern are, as yet unknown, negative effects on the immune system. In the 0-4s trial, only seven children were described as having “severe” COVID-19 – six vaccinated and one given placebo. Similarly, for the 12 children with recurrent episodes of infection, 10 were vaccinated against only two who received placebo. These are all tiny figures and much too small to rule out any adverse impacts such as antibody-dependent enhancement (ADE) and other impacts on the immune system.
- Also unanswered is the question of Original Antigenic Sin. It is of note that in a large Israeli study, those infected after vaccination had poorer cover than those vaccinated after infection. In the Moderna trial, N-antibodies were seen in only 40% of those infected after vaccination, compared with 93% of those infected after placebo.
- There is evidence of vaccine-induced disruption of both innate and adaptive immune responses. The possibility of developing an impaired immune function would be disastrous for children, who have the most competent innate immunity, which by now has been effectively trained by the circulating virus.
- The unknown is whether there will be any adverse effect on T-cell function leading to an increase in cancers.
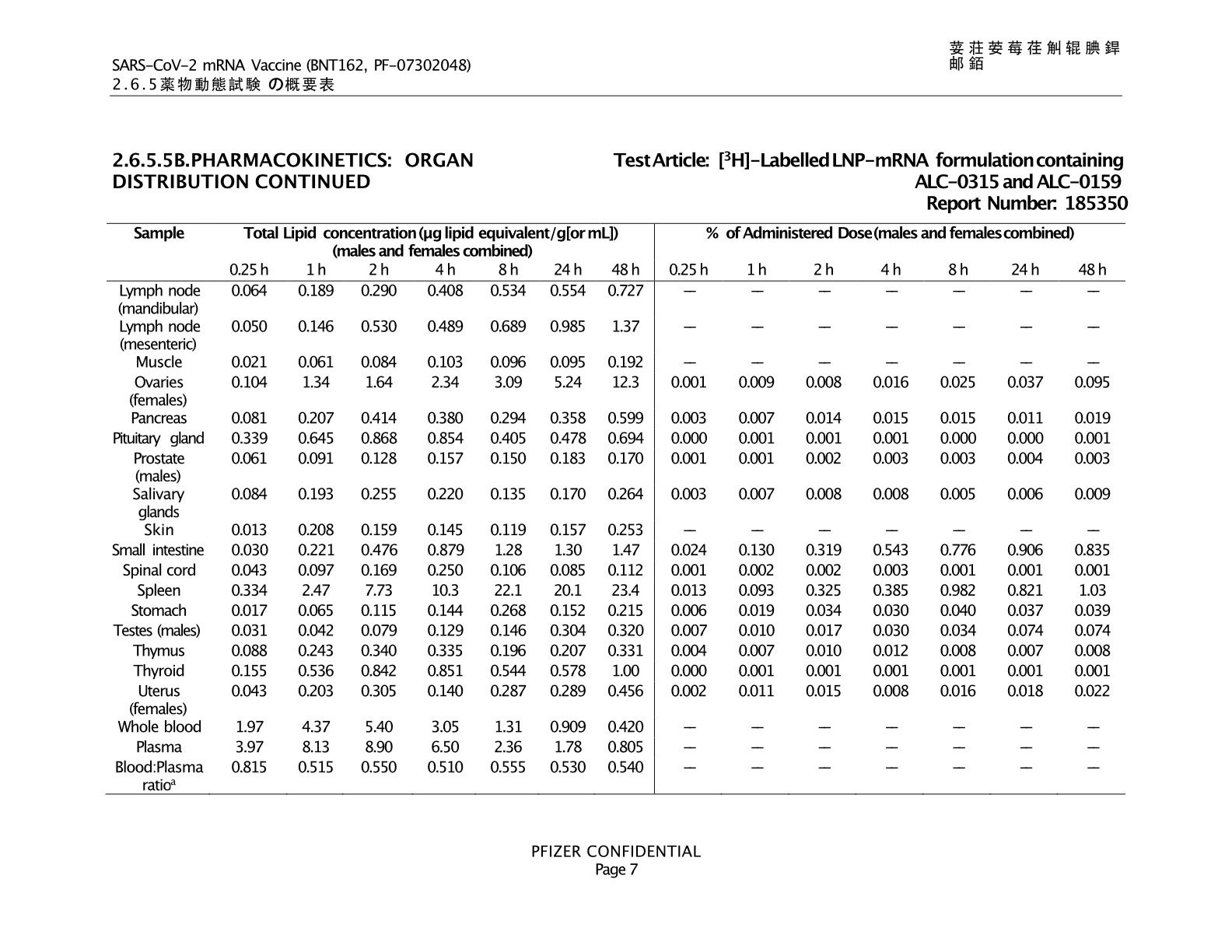
- Also, in terms of reproductive function, limited animal bio-distribution studies showed lipid nanoparticles concentrate in ovaries and testes. Adult sperm donors have shown a reduction in sperm counts particularly of motile sperm, falling by three months post-vaccination and remaining depressed at four to five months.
- Even for adults, concerns are rising that serious adverse events are more than hospitalizations from COVID-19.
D. Informed consent
- For 5-11s, the JCVI, in recommending a “non-urgent offer” of vaccination, specifically noted the importance of fully informed consent with no coercion.
- With the low uptake in this age group, the presence of ‘therapy dogs’, advertisements including superhero images and information about child vaccination protecting friends and family all clearly run contrary to the concept of consent, fully informed and freely given.
- The complete omission of information explaining to the public the different and novel technology used in COVID-19 vaccines compared to standard vaccines, and the failure to inform of the lack of any long-term safety data, borders on misinformation.
E. Effect on public confidence
- Vaccines against much more serious diseases, such as polio and measles, need to be prioritized. Pushing an unnecessary and novel, gene-based vaccine onto young children risks seriously undermining parental confidence in the whole immunization program.
- The poor quality of the data presented by Pfizer risks bringing the pharmaceutical industry into disrepute and the regulators if this product is authorized.
In summary, young healthy children are at minimal risk from COVID-19, especially since the arrival of the Omicron variant. Most have been repeatedly exposed to SARS-CoV-2 virus, yet have remained well, or have had short, mild illness. As detailed above, the vaccines are of brief efficacy, have known short- to medium-term risks and unknown long-term safety. Data for clinically useful efficacy in small children are scant or absent. In older children, for whom the vaccines are already licensed, they have been promoted via ethically dubious schemes to the potential detriment of other, and vital, parts of the childhood vaccination program.
For a tiny minority of children for whom the potential for benefit clearly and unequivocally outweighed the potential for harm, vaccination could have been facilitated by restrictive licenses. Whether following the precautionary principle or the instruction to First Do No Harm, such vaccines have no place in a routine childhood immunization program.
(Signed):
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMed Sci, Principal, Institute for Cancer Vaccines & Immunotherapy (ICVI)
Professor Anthony Fryer, PhD, FRCPath, Professor of Clinical Biochemistry, Keele University
Professor David Livermore, BSc, PhD, Retired Professor of Medical Microbiology, UEA
Professor John Fairclough FRCS FFSEM retired Honorary Consultant Surgeon
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, House of Lords, former Parliamentary Under-Secretary of State 2001-2003, formerCconsultant in Public Health Medicine
Dr Abby Astle, MA(Cantab), MBBChir, GP Principal, GP Trainer, GP Examiner
Dr Michael D Bell, MBChB, MRCGP, retired General Practitioner
Dr Alan Black, MBBS, MSc, DipPharmMed, Retired Pharmaceutical Physician
Dr David Bramble, MBChB, MRCPsych, MD, Consultant Psychiatrist
Dr Emma Brierly, MBBS, MRCGP, General Practitioner
Dr David Cartland, MBChB, BMedSci, General practitioner
Dr Peter Chan, BM, MRCS, MRCGP, NLP, General Practitioner, Functional medicine practitioner
Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational Health Practitioner
Julie Coffey, MBChB, General Practitioner
John Collis, RN, Specialist Nurse Practitioner, retired
Mr Ian F Comaish, MA, BM BCh, FRCOphth, FRANZCO, Consultant Ophthalmologist
James Cook, NHS Registered Nurse, Bachelor of Nursing (Hons), Master of Public Health
Dr Clare Craig, BMBCh, FRCPath, Pathologist
Dr David Critchley, BSc, PhD in Pharmacology, 32 years experience in Pharmaceutical R&D
Dr Jonathan Engler, MBChB, LLB (Hons), DipPharmMedDr Elizabeth Evans, MA (Cantab), MBBS, DRCOG, Retired Doctor
Dr John Flack, BPharm, PhD, retired Director of Safety Evaluation at Beecham Pharmaceuticals and retired Senior Vice-president for Drug Discovery SmithKline Beecham
Dr Simon Fox, BSc, BMBCh, FRCP, Consultant in Infectious Diseases and Internal Medicine
Dr Ali Haggett, Mental health community work, 3rd sector, former lecturer in the history of medicine
David Halpin, MB BS FRCS, Orthopaedic and trauma surgeon (retired)
Dr Renée Hoenderkampf, General Practitioner
Dr Andrew Isaac, MB BCh, Physician, retired
Dr Steve James, Consultant Intensive Care
Dr Keith Johnson, BA, DPhil (Oxon), IP Consultant for Diagnostic Testing
Dr Rosamond Jones, MBBS, MD, FRCPCH, retired consultant paediatrician
Dr Tanya Klymenko, PhD, FHEA, FIBMS, Senior Lecturer in Biomedical Sciences
Dr Charles Lane, MA, DPhil, Molecular Biologist
Dr Branko Latinkic, BSc, PhD, Molecular Biologist
Dr Felicity Lillingstone, IMD DHS PhD ANP, Doctor, Urgent Care, Research Fellow
Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd, Bath
Katherine MacGilchrist, BSc (Hons), MSc, CEO/Systematic Review Director, Epidemica Ltd.
Dr Geoffrey Maidment, MBBS, MD, FRCP, Consultant Physician, retired
Ahmad K Malik FRCS (Tr & Orth) Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
Dr Kulvinder Singh Manik, MBBS, General Practitioner
Dr Fiona Martindale, MBChB, MRCGP, General Practitioner
Dr S McBride, BSc (Hons) Medical Microbiology & Immunobiology, MBBCh BAO, MSc in Clinical Gerontology, MRCP(UK), FRCEM, FRCP (Edinburgh). NHS Emergency Medicine & Geriatrics
Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
Dr Franziska Meuschel, MD, ND, PhD, LFHom, BSEM, Nutritional, Environmental and Integrated Medicine
Dr Scott Mitchell, MBChB, MRCS, Emergency Medicine Physician
Dr Alan Mordue, MBChB, FFPH. Retired Consultant in Public Health Medicine & Epidemiology
Dr David Morris, MBChB, MRCP(UK), General Practitioner
Margaret Moss, MA (Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Dr Alice Murkies, MD FRACGP MBBS, General Practitioner
Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
Dr Sarah Myhill, MBBS, retired GP and Naturopathic Physician
Dr Rachel Nicholl, PhD, Medical researcher
Dr Christina Peers, MBBS, DRCOG, DFSRH, FFSRH, Menopause specialist
Rev Dr William J U Philip MB ChB, MRCP, BD, Senior Minister The Tron Church, Glasgow, formerly physician specialising in cardiology
Dr Angharad Powell, MBChB, BSc (hons), DFRSH, DCP (Ireland), DRCOG, DipOccMed, MRCGP, General Practitioner
Dr Gerry Quinn, PhD. Postdoctoral researcher in microbiology and immunology
Dr Johanna Reilly, MBBS, General Practitioner
Jessica Righart, MSc, MIBMS, Senior Critical Care Scientist
Mr Angus Robertson, BSc, MB ChB, FRCSEd (Tr & Orth), Consultant Orthopaedic Surgeon
Dr Jessica Robinson, BSc(Hons), MBBS, MRCPsych, MFHom, Psychiatrist and Integrative Medicine Doctor
Dr Jon Rogers, MB ChB (Bristol), Retired General Practitioner
Mr James Royle, MBChB, FRCS, MMedEd, Colorectal surgeon
Dr Roland Salmon, MB BS, MRCGP, FFPH, Former Director, Communicable Disease Surveillance Centre Wales
Sorrel Scott, Grad Dip Phys, Specialist Physiotherapist in Neurology, 30 years in NHS
Dr Rohaan Seth, BSc (hons), MBChB (hons), MRCGP, Retired General Practitioner
Dr Gary Sidley, retired NHS Consultant Clinical Psychologist
Dr Annabel Smart, MBBS, retired General Practitioner
Natalie Stephenson, BSc (Hons) Paediatric Audiologist
Dr Zenobia Storah,MA (Oxon), Dip Psych, DClinPsy, Senior Clinical Psychologist (Child and Adolescent)
Dr Julian Tompkinson, MBChB MRCGP, General Practitioner GP trainer PCME
Dr Noel Thomas, MA, MBChB, DCH, DObsRCOG, DTM&H, MFHom, retired doctor
Dr Stephen Ting, MB CHB, MRCP, PhD, Consultant Physician
Dr Livia Tossici-Bolt, PhD, Clinical Scientist
Dr Carmen Wheatley, DPhil, Orthomolecular Oncology
Dr Helen Westwood MBChB MRCGP DCH DRCOG, General Practitioner
Mr Lasantha Wijesinghe, FRCS, Consultant Vascular Surgeon
Dr Damian Wilde, PhD, (Chartered) Specialist Clinical Psychologist
Dr Ruth Wilde, MB BCh, MRCEM, AFMCP, Integrative & Functional Medicine Doctor